Skip to content
Keyboard Accessible Menu
Skip to content
Home
About
Mission and Goals
Dr. Jason Reeder
Dr. Gretchen Kuchenmeister
Meet Our Staff
Clients
New Client Form
Canine
What to Expect At Your Dog’s Appointment
Your Dog’s Procedure
At Home Care For Dogs After Procedure
Anesthesia and Monitoring For Dogs
Feline
What to Expect at Your Cat’s Appointment
Your Cat’s Procedure
At Home Care For Your Cat After Procedure
Anesthesia And Monitoring For Cats
Benefits of Minimally Invasive Procedures
Policies and Procedures
Referring Veterinarians
Interventional Radiology and Endoscopy Procedures
Referral Form
Procedures
Contact Us/Hours
Employment
Home
About
Mission and Goals
Dr. Jason Reeder
Dr. Gretchen Kuchenmeister
Meet Our Staff
Clients
New Client Form
Canine
What to Expect At Your Dog’s Appointment
Your Dog’s Procedure
At Home Care For Dogs After Procedure
Anesthesia and Monitoring For Dogs
Feline
What to Expect at Your Cat’s Appointment
Your Cat’s Procedure
At Home Care For Your Cat After Procedure
Anesthesia And Monitoring For Cats
Benefits of Minimally Invasive Procedures
Policies and Procedures
Referring Veterinarians
Interventional Radiology and Endoscopy Procedures
Referral Form
Procedures
Contact Us/Hours
Employment
(503) 567-8835
19056 Willamette Drive
West Linn, OR 97068
Referral Form
Referral Form
This form is to be completed by the referring veterinarian. Please clear your browsing history before completing the form.
Marked Fields Are Required
Instagram
This field is for validation purposes and should be left unchanged.
Client Information
Client Name
(Required)
First
Last
Client Address
Client Primary Phone
(Required)
Client Preferred Email
(Required)
Veterinarian Information
Referring Veterinarian
(Required)
Referring Hospital
(Required)
Address
Referring Veterinarian Phone
(Required)
Fax
Referring Veterinarian Email
(Required)
Other primary or consulting veterinarians and clinics
(Required)
Patient Information
Patient Name
(Required)
Species
(Required)
Dog
Cat
Date of Birth or Approximate Age
(Required)
Breed
(Required)
Gender
(Required)
Intact male
Neutered male
Intact female
Spayed female
Body weight (indicate lbs or kgs)
(Required)
Referral Information
Consult requested with
(Required)
Dr. Kuchenmeister (Soft Tissue Surgery)
Dr. Reeder (Internal Medicine)
Both
Pertinent medical history
(Required)
Differential diagnoses
(Required)
Completed diagnostic tests
CBC
Chemistry profile
Thyroid testing
Other bloodwork (specify)
Urinalysis
Radiographs
Diagnostic ultrasound
Culture
Cytology
Histopathology
CT
MRI
Echocardiography
Other imaging studies (specify)
Specify what other blood work
(Required)
Specify what other imaging studies
(Required)
Current medications
(Required)
Current diet
(Required)
Services/procedures requested
(Required)
Today's Date
(Required)
Month
Month
1
2
3
4
5
6
7
8
9
10
11
12
Day
Day
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
Year
Year
2027
2026
2025
2024
2023
2022
2021
2020
2019
2018
2017
2016
2015
2014
2013
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
1988
1987
1986
1985
1984
1983
1982
1981
1980
1979
1978
1977
1976
1975
1974
1973
1972
1971
1970
1969
1968
1967
1966
1965
1964
1963
1962
1961
1960
1959
1958
1957
1956
1955
1954
1953
1952
1951
1950
1949
1948
1947
1946
1945
1944
1943
1942
1941
1940
1939
1938
1937
1936
1935
1934
1933
1932
1931
1930
1929
1928
1927
1926
1925
1924
1923
1922
1921
1920
Medical Records
Please submit all previous medical records, including all chart notes, diagnostic test results, and images, either by uploading here or emailing to records@miscaspecialtyvet.com
Drop files here or
Select files
Max. file size: 80 MB.
CAPTCHA
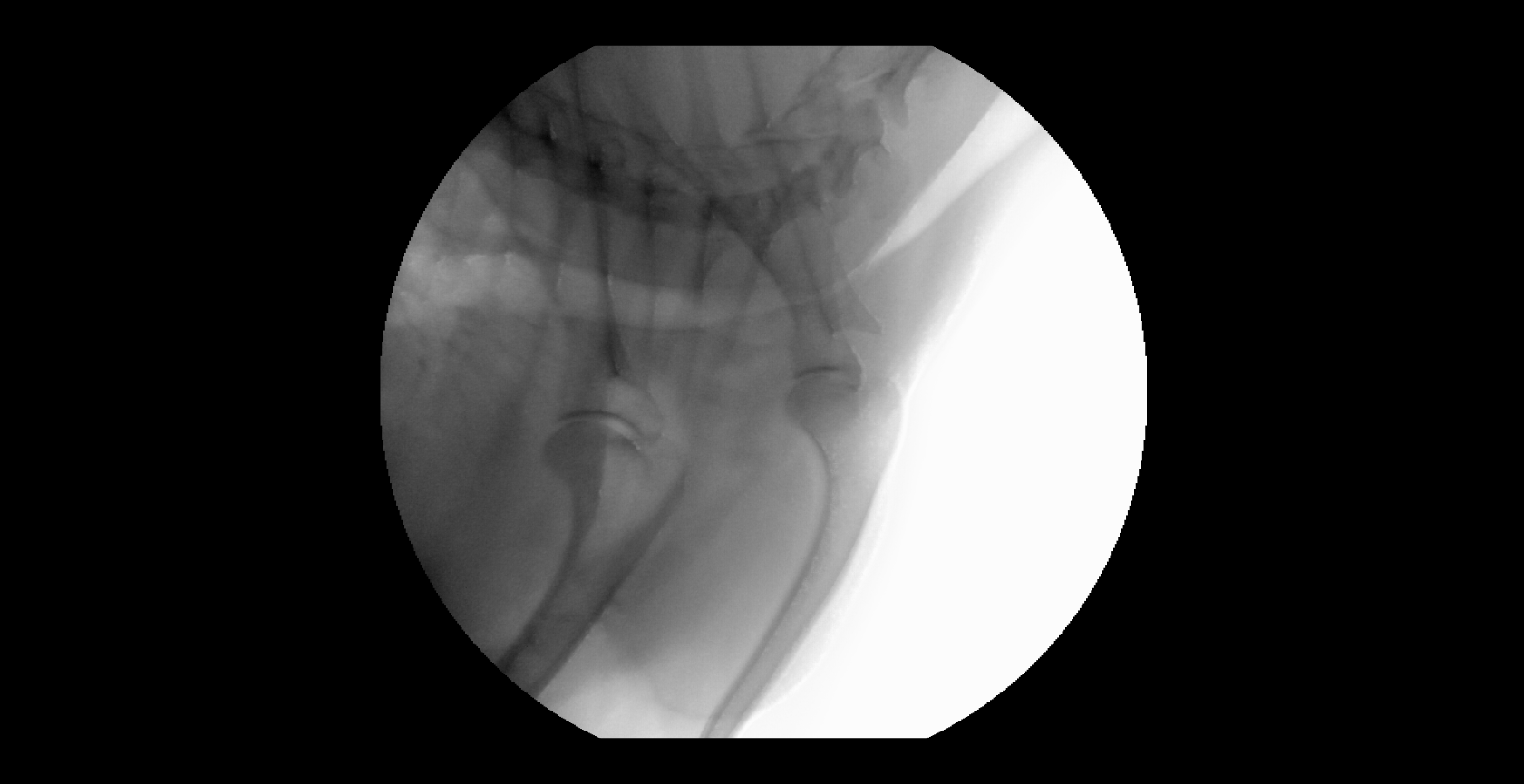
Pre Stent
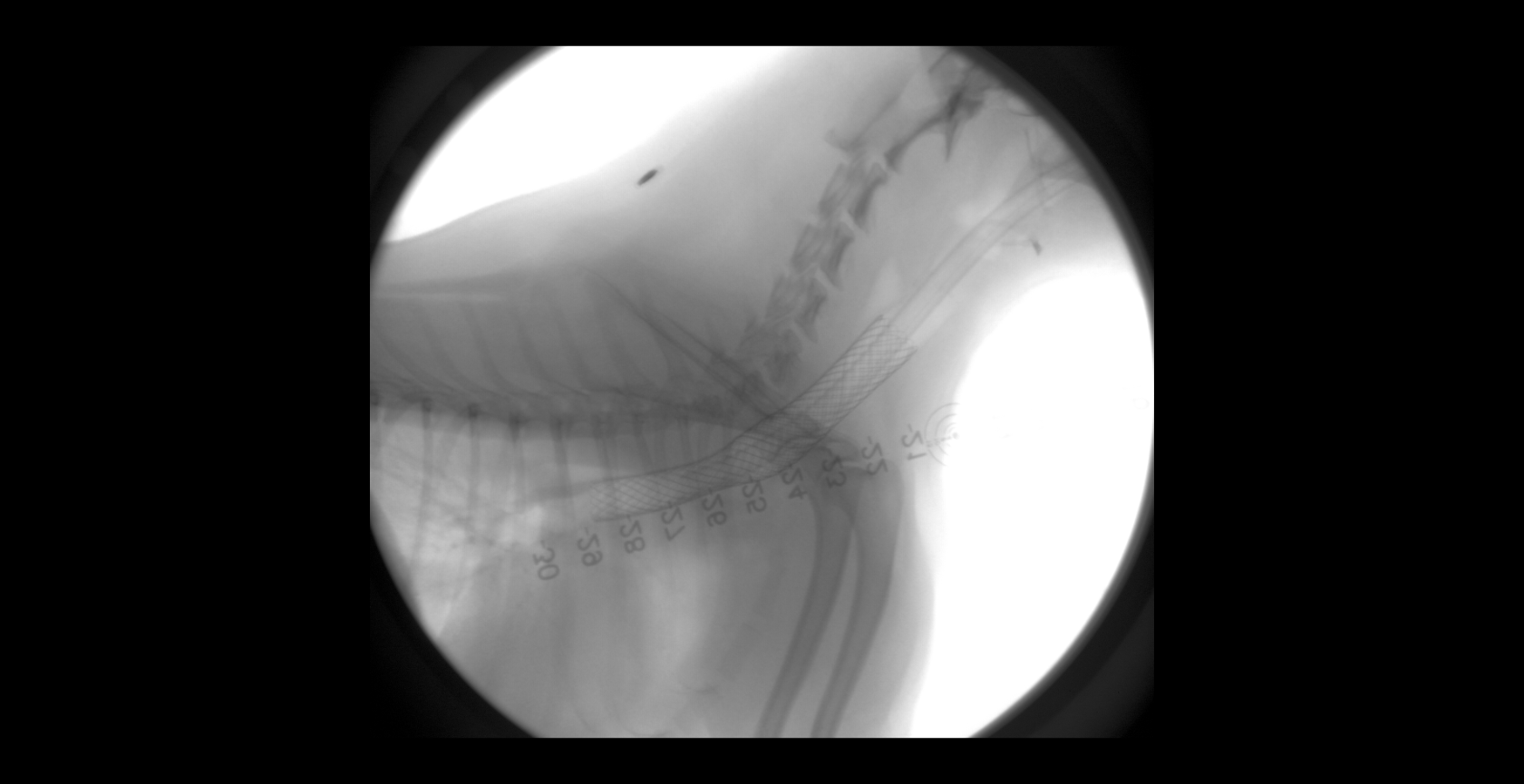
Post Balloon
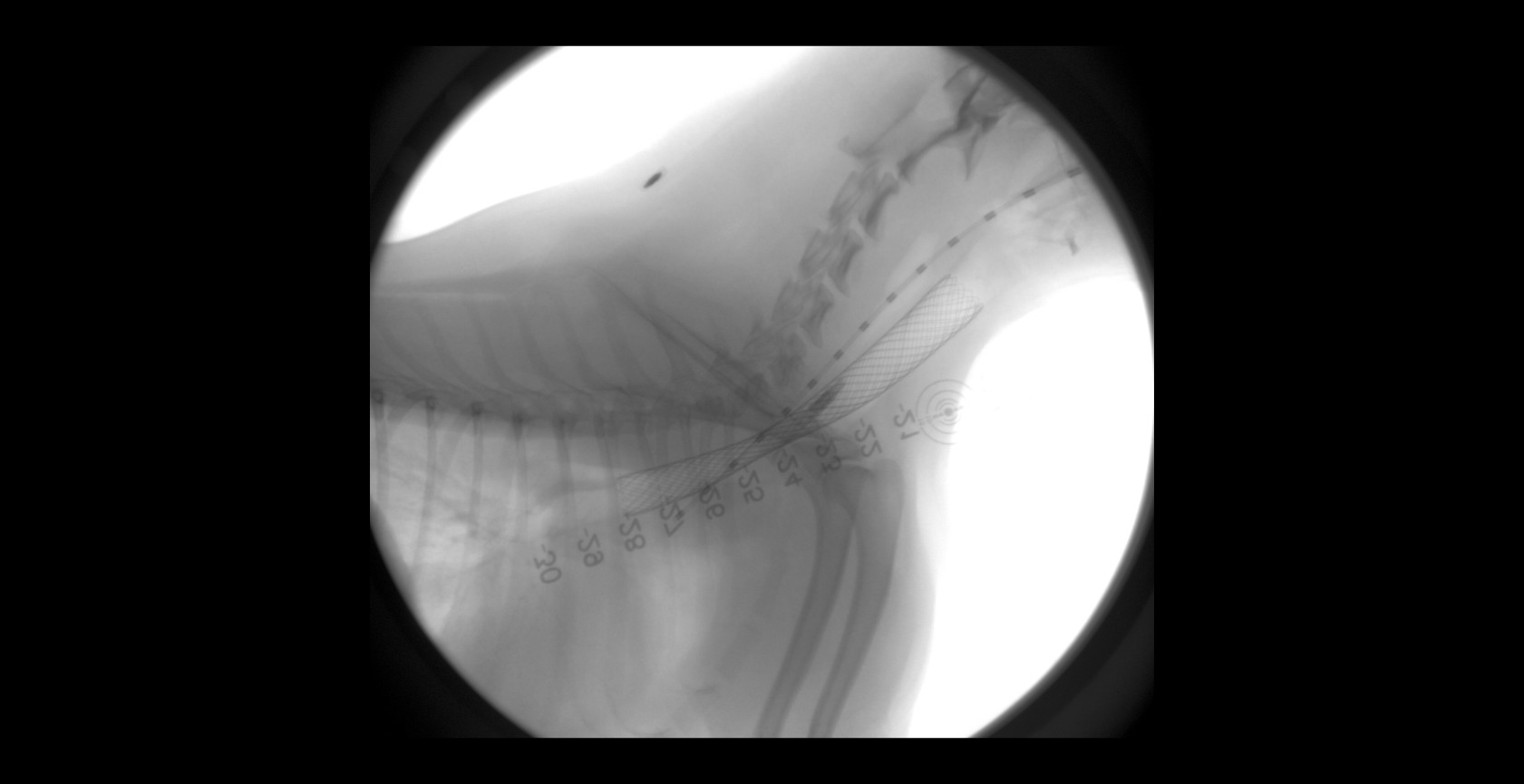
Pre Balloon