
Percutaneous Transvenous Coil Embolization (PTCE)
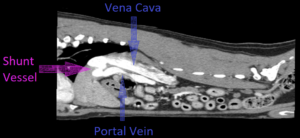
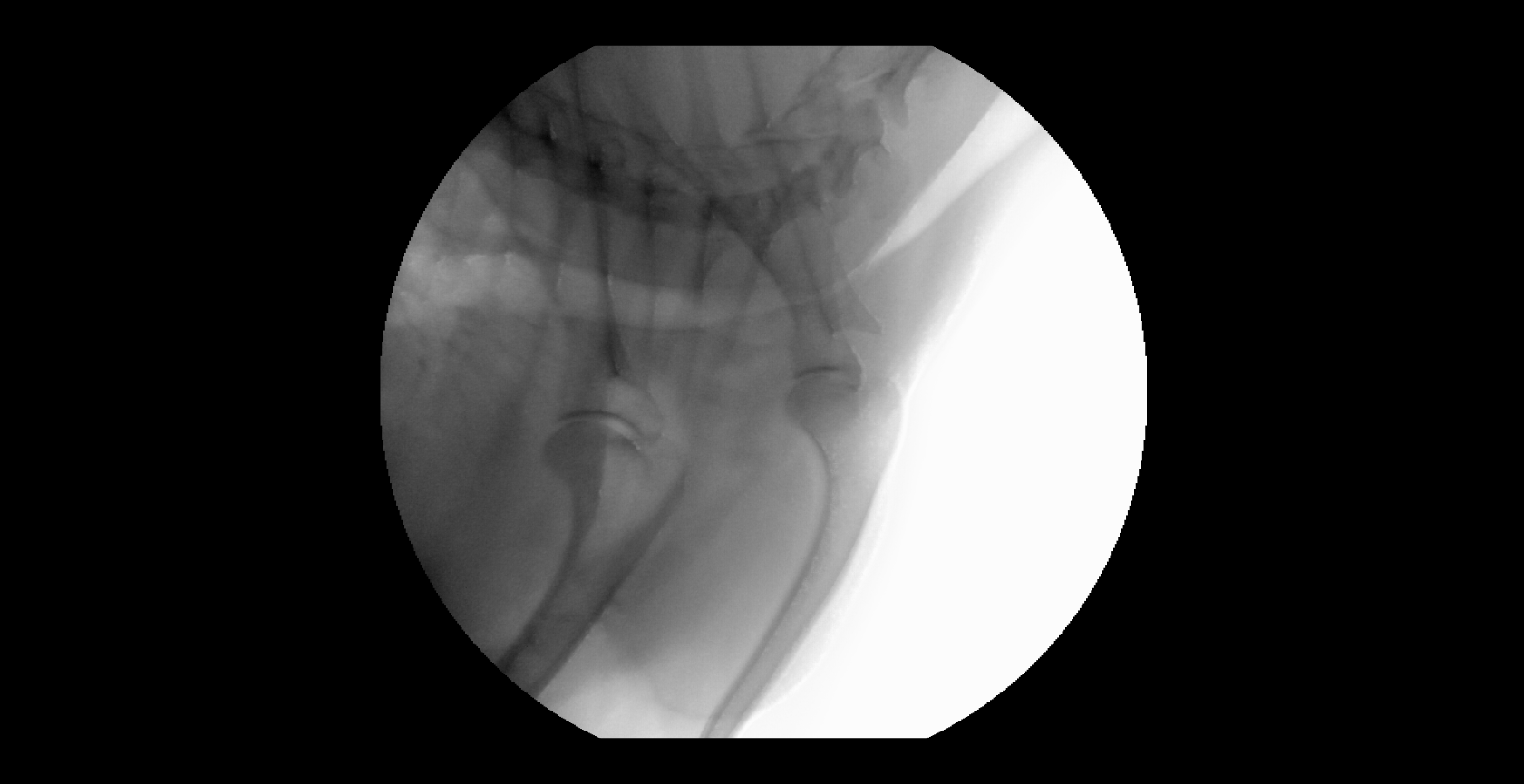
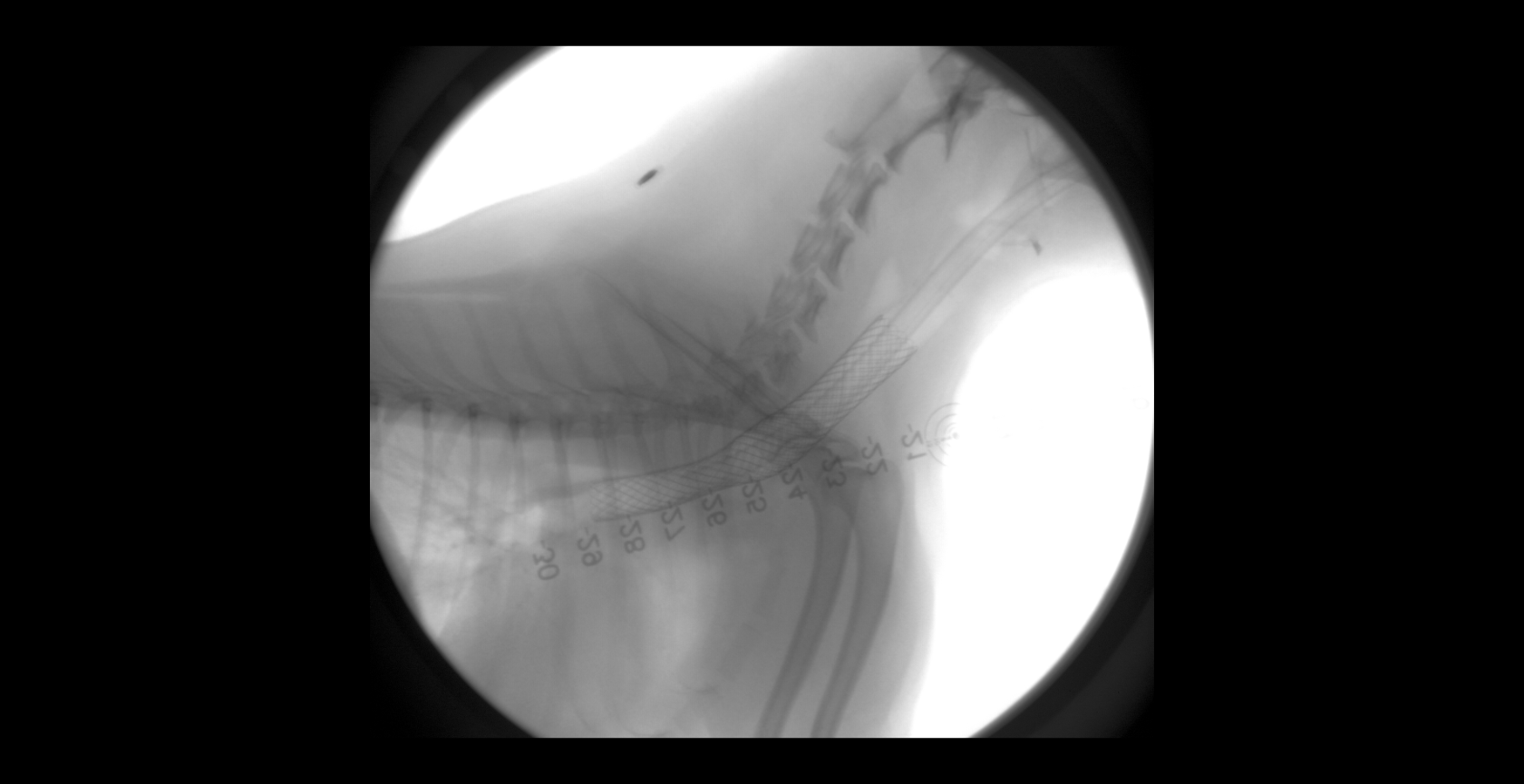
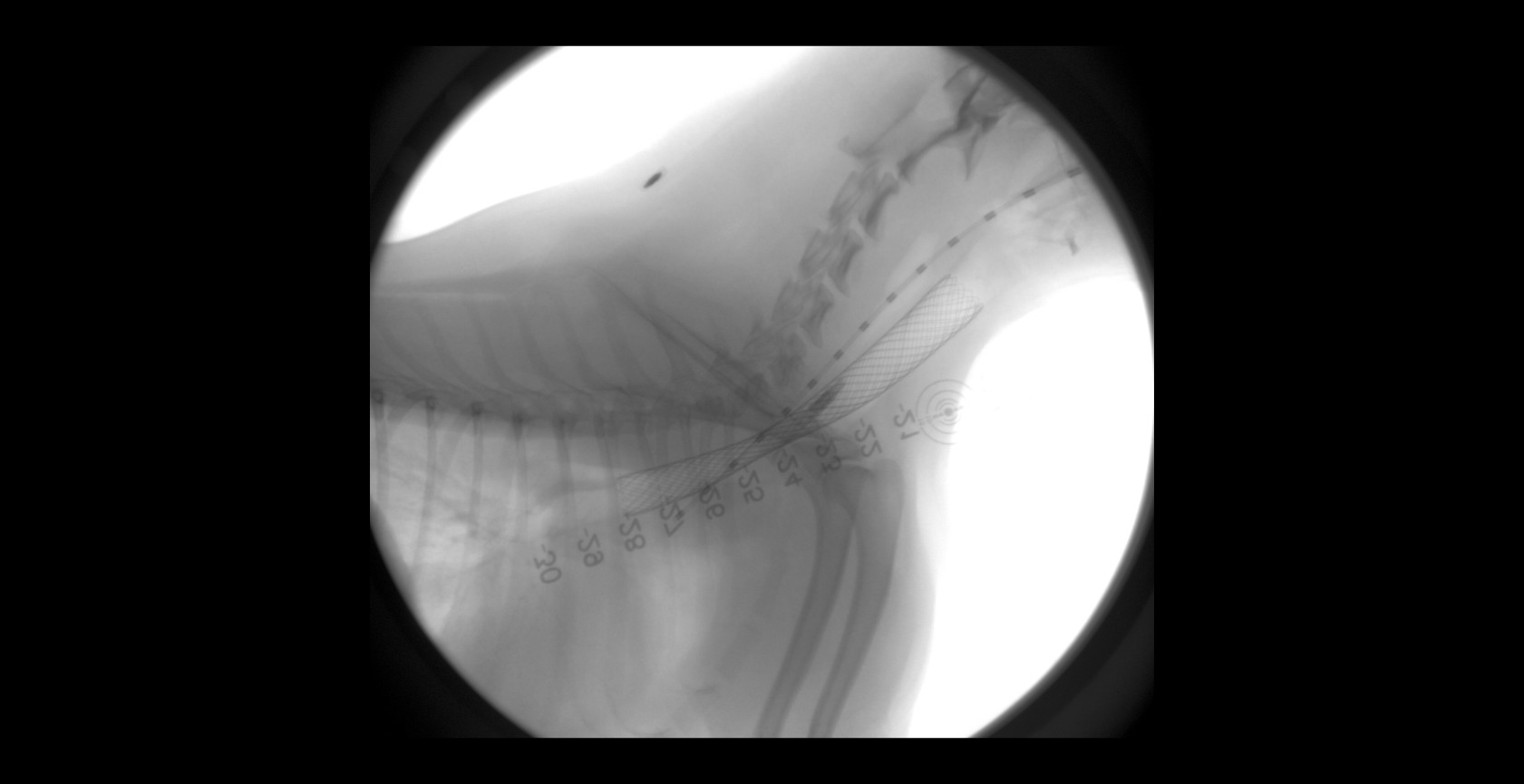
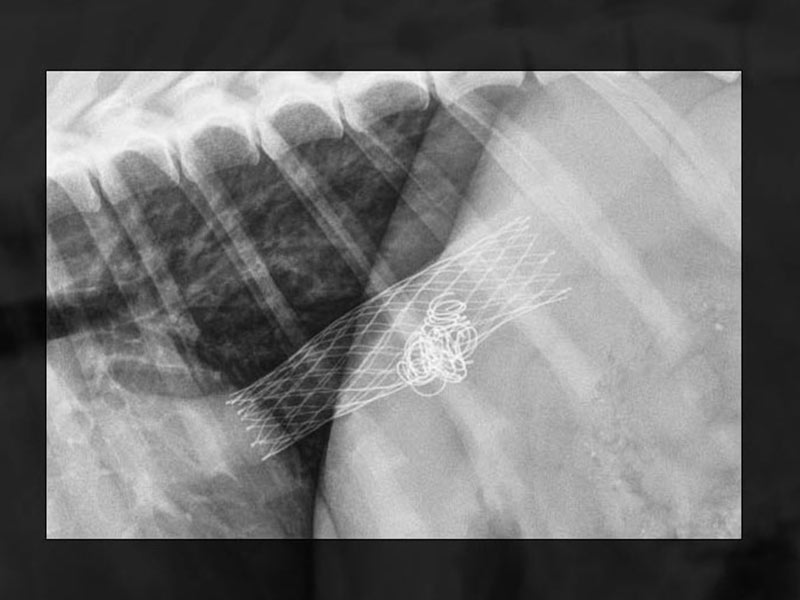
Portosystemic shunts are relatively uncommon congenital vascular anomalies that shunt blood from the abdominal organs around the liver and to the heart, thereby preventing detoxification of the shunted blood. Percutaneous transvenous coil embolization (PTCE) is a minimally invasive procedure using fluoroscopy to place intravenous coils to occlude the shunt vessel. PTCE results in a faster recovery, better outcome, reduced complications, and less mortality.

{kind=link}
{kind=link}
{kind=link}